Prescription for disaster: America's broken pharmacy system in revolt over burnout and errors
Pharmacists with the nation’s largest retail pharmacy chain felt dangerously burned out.
It was August 2020. The pandemic was in full swing, straining an already weary workforce hit by a decade of relentless budget cuts and rising demands.
One by one, the pharmacists dialed into a weekly conference call with their boss. He could have empathized with them or addressed the reality of their pressure-cooker environment – one that breeds medication errors and creates missed opportunities to prevent potentially deadly mistakes.
Instead, CVS District Leader Khalil Haidar turned up the heat. He harped on his Texas-and-Louisiana-based team to hit corporate quotas: Sell more store memberships. Push for more prescription pickups. Vaccinate more people. He threatened discipline and staff cuts unless pharmacists convinced at least five customers that week to get a flu shot before flu season had even officially started.
“If you get your goal, nobody will come after you," Haidar said on the call, one of several recorded and shared with USA TODAY. "And many patients, they are ignorant. They don’t know what the flu is ... How are you going to convince them? How can you persuade them? That’s your job as a pharmacist.”
Pharmacists take an oath to hold patient safety in the highest regard when preparing and dispensing medication. But rising pressures inside the nation’s largest retail chains have forced pharmacists to choose between that oath and their job.
The situation was bad before the pandemic. COVID-19 made it worse. It has only gone downhill since then. Frustrations boiled over this autumn in a series of high-profile walkouts that left a string of CVS and Walgreens pharmacies shuttered or short-staffed. Those actions might have caught consumers off guard. But inside the troubled industry, it was the clarion call of a beleaguered workforce pushed to the brink.
Corporations like CVS, Rite Aid, Walgreens and Walmart have consistently slashed pharmacy staffing levels while simultaneously saddling their frontline workers with a burgeoning list of additional duties.
Stores that a decade ago might have had two pharmacists and six pharmacy technicians filling an average of 500 prescriptions a day now may have half the staff and an even higher prescription volume – plus an endless crush of vaccine appointments, rapid tests and patient consultation calls.
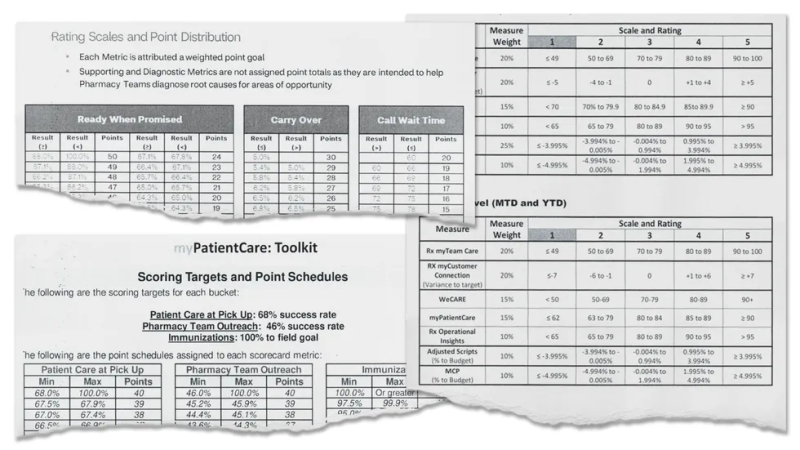
Every task is timed and measured against corporate goals that reward speed and profits. Staff who do not fill prescriptions fast enough, answer the phones quickly enough or drum up enough vaccination business can face discipline, reassignment or termination.
Pharmacists said it’s nearly impossible to meet all the demands without cutting corners, and when corners get cut, patients can get hurt.
“The public’s health is in danger,” said Oklahoma City pharmacist Bled Tanoe, who quit her job at Walgreens in August 2021 over what she considered unsafe staffing levels and an emphasis on hitting corporate targets. “The incidents of error are multiplied by infinity.”

USA TODAY interviewed four dozen current and former retail pharmacists from different chains across the nation and spoke with industry leaders, patient advocates and patients harmed by pharmacy errors. Many pharmacists spoke to USA TODAY on the condition of anonymity to protect their jobs.
The media organization also reviewed more than 100 emails from chain pharmacists sharing their concerns; inspected internal emails, text messages, metric score sheets and coaching notes; and listened to more than five hours of recorded conference calls.
These interviews, audio recordings and documents – along with dozens of pharmacist workplace surveys, task force studies and state board of pharmacy reports – add up to a prescription for disaster.
“I could cry as to what’s happening in my profession,” said Daniel A. Hussar, a professor and dean emeritus at the Philadelphia College of Pharmacy, where he taught for 52 years before retiring in 2018 to focus on his family and his blog, The Pharmacist Activist.
Hussar lamented the transformation of a once-vaunted career into the equivalent of a fast-food job whose workers are pressured to upsell every customer and race through every order. Mistakes in that environment are not only common, he said, they’re potentially fatal.
“At corporations like CVS, Walgreens, Walmart, Rite Aid – the huge pharmacies – errors are a cost of doing business,” Hussar said. “I don’t think the boards of pharmacy or the colleges of pharmacy or the professional associations are doing enough to address the issues.”
For years, pharmacists have reported these problems to their state boards, complained to their professional organizations and warned the media. The New York Times wrote about how the dangerous workload imperils patient safety just before the pandemic hit U.S. shores.
Promises were made and broken – documented by pharmacists themselves in state surveys that followed.
In California, 91% of chain pharmacists surveyed by the state Board of Pharmacy in 2021 said they lacked the staff needed to ensure adequate patient care. More than half of pharmacists polled by the Kansas Board of Pharmacy in 2022 said they didn’t feel they could perform their jobs safely; the biggest reasons cited were a lack of adequate staffing and employer-imposed metrics, like filling a specific number of prescriptions a day or providing service to customers within a set time.
Hundreds of pharmacists in Ohio responded to a 2020 callout from their state board about the toll of their workload on patient safety in a report made public in the next year.
“I feel a mistake is breathing down my neck as I try to manage all the tasks that I am asked to perform,” one wrote. Another said they had left the profession because “the environment was set up for me to fail.”
State regulatory bodies overseeing pharmacies have for years refused to intervene. Their role is mainly to protect consumers, not pharmacists, and they traditionally considered many of these complaints – staffing, metrics, workload – outside their purview. They were seen as business decisions, not consumer safety issues, said Karen Winslow, interim executive director of the Virginia Pharmacy Association.
That’s starting to change, but not without a fight.
Ohio proposed a series of rules this year aimed at improving pharmacy working conditions. Among them: A ban on quotas and requirements for sufficient staffing. The rules are currently pending a vote amid overwhelming support from pharmacists and opposition from retail pharmacy chains, including Walgreens and CVS.
“The Board should stay focused on the regulation of the practice of pharmacy rather than the business of pharmacy,” wrote CVS Director of Regulatory Affairs John Long in opposing an early version of Ohio’s rules last year.
Virginia passed emergency regulations in late September also banning production quotas and bolstering pharmacy staffing. Those rules are in effect until March 2025, giving the state time to develop and pass more permanent measures.
Enforcing these rules could prove challenging. California, one of the first states to outlaw pharmacy production quotas and mandate minimum staffing, is coping with routine violations by retail pharmacies that then fail to provide records to inspectors seeking to verify complaints, state Board of Pharmacy minutes show.
Professional associations, meanwhile, have earned their members’ scorn for hosting workshops on resiliency rather than advocating for better working conditions. Many pharmacists told USA TODAY they feel like no one stands up for them.
That, too, is starting to change. In the wake of the CVS walkouts last month, the new head of the American Pharmacists Association, the industry’s largest professional organization, flew to Kansas City to meet with the organizers and committed to more aggressive leadership on these issues.
“The APhA has been focused on longer-term fixes, and what we’ve heard loud and clear is we need to focus on the acute problems,” said Michael Hogue, the association’s chief executive officer and executive vice president. “That’s what we’re going to do.”
USA TODAY reached out to CVS, Walgreens, Walmart and Rite Aid for comment.
Representatives of CVS and Walgreens generally acknowledged the challenges their pharmacists have faced in recent years but denied allegations of dangerous working conditions. They said goal-based metrics on measurable objectives such as quick prescription turnarounds, short telephone hold times and vaccination volumes are standard within the industry and meant to assess quality rather than penalize staff.
CVS, Rite Aid, Walgreens and Walmart all emphasized their commitments to patient safety and described their various efforts to continually reduce error rates.
“Patient safety is our highest priority,” Amy Thibault, CVS Pharmacy’s lead director of external communications, told USA TODAY. “Our more than 30,000 CVS pharmacists approach this responsibility with seriousness and dedication and we work hard to earn the trust of our pharmacy patients.”
CVS, Walgreens and Walmart also said they have invested in new technologies to streamline services, increased wages to better recruit and retain staff, and rolled out new initiatives to support their teams and reduce their workloads.
The major chains now provide half-hour lunch breaks for staff. Many also recently announced reduced pharmacy hours at locations nationwide. Walmart spokesman Tyler Thomason said reduced operating hours promote a “better work/life balance.”
But pharmacists told USA TODAY their workloads remain the same and that they’re pressured to work through lunch and stay late to finish everything. At locations where hours were cut, many pharmacists said, they’ve seen their salaries decrease accordingly.
“I’ve given the company thousands and thousands of dollars in free labor,” said a CVS pharmacist who was on Haidar’s team during the pandemic-era conference calls. “Our bosses can log into the computer any time and tell how far behind we are. They will send group texts and say, ‘I see you’re trending behind. What are your plans to finish it tonight?’ Very intimidating comments. You fear for your job all the time.”
Haidar, who now leads a different team, told USA TODAY the recordings must have been altered and that he never threatened staff with discipline for falling short of vaccination goals. He also said they are not an accurate depiction of his leadership. When asked if he would like to listen to the recordings, Haidar declined.
Michael DeAngelis, CVS’ executive director of corporate communications, said it is not the company’s “policy or practice to penalize pharmacy teams regarding the number of vaccinations they administer” and that it “is committed to compensating our colleagues appropriately for the hours they work.”
DeAngelis also said CVS recently reduced its pharmacy metrics by 50%, but he declined to provide additional details.
Walgreens announced last year the complete elimination of performance-based metrics, the only major chain to have taken such a step. But interviews with pharmacists and documents provided to USA TODAY show the company continues to push staff to hit unrealistic goals.
One Walgreens pharmacist said she was reprimanded earlier this month for taking too long to verify prescriptions, even though her extra diligence had caught several serious mistakes.
According to notes from her coaching session, shared with USA TODAY, she should take less than 30 seconds to verify the accuracy and appropriateness of every prescription, in addition to checking for potential problems like drug allergies or interactions.
“I pray every day that I don’t miss something or cause a patient harm,” said the Tennessee-based pharmacist, who estimates she handles several hundred prescriptions daily. “I feel guilty knowing that I would want someone to double check the math on a prescription of antibiotics for my child, but I don’t have time to do that for their child.”
Medication errors: A pharmacist's worst nightmare
Medication errors are a pharmacist’s worst nightmare. Many told USA TODAY they lie awake at night wondering if, in their haste, they made a mistake that might hurt or kill someone.
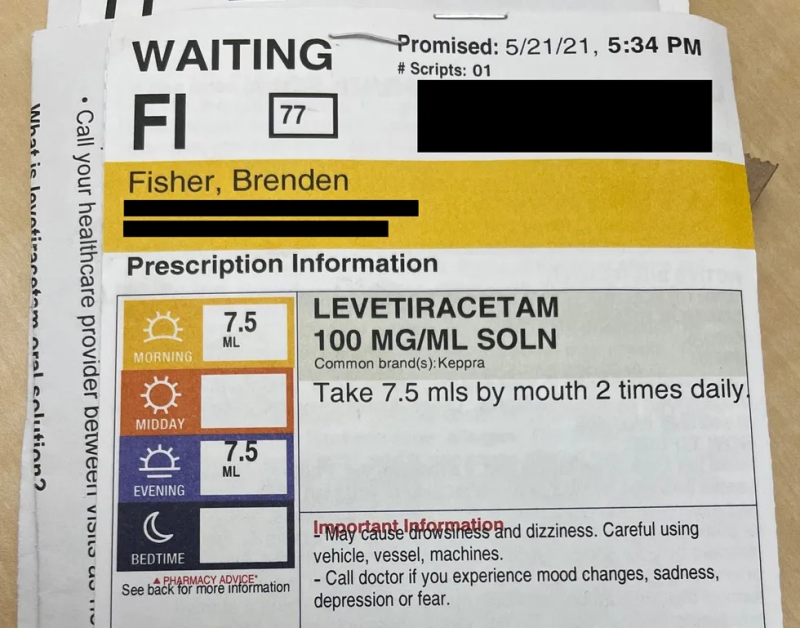
In May 2021, that someone was Brenden Fisher.
The Sarasota, Florida, child overdosed on a newly prescribed anti-seizure medication after the CVS pharmacy near his home dispensed the drug with the wrong instructions on the label.

By the third dose, Brenden was lethargic, dazed and struggling to breathe. His parents, Paris Bean and Jason Fisher, rushed their then-2-year-old to the hospital, thinking he was dying.
Hospital staff didn’t know what was wrong with him, Bean recalled, until a nurse asked if he was taking his 1.2 ml of levetiracetam twice daily.
When Bean told her the instructions said to give him 7.5 ml, “you could almost hear her jaw drop,” Bean recalled. “She said, ‘Did you give that to him?’ And I said, ‘Yes. Is that why we’re here?’ She said, ‘I wouldn’t be surprised.’”
Brenden still suffers from a full-body tic he first developed during the incident, his parents said. Dozens of times a day, he will suddenly stop whatever he is doing, clasp his hands together, clench his jaw and tense every muscle in his body while staring off into space. Each episode lasts anywhere from 5-10 seconds.
His parents haven’t been able to definitively link the tic to the overdose, but they said they have no other explanation for it.
Anti-seizure medications like levetiracetam depress the central nervous system, Hussar said. Because nerves tell muscles when to contract and relax, he said, there could be a connection between the overdose and Brenden’s involuntary muscle contractions.
Bean said she blames CVS for the mistake but also herself: “I’m the one who physically administered it ... I could have killed him.”
CVS declined to comment on the error.
Bean and her husband filed a lawsuit against CVS in February that was settled out of court for an undisclosed sum. But they said they did not file a complaint with the Florida Board of Pharmacy.
That means it’s one of countless errors for which there’s no official tally or public record.

Despite a widespread industry belief that medication errors are on the rise as a result of unsafe working conditions, there is no reliable or comprehensive public data to prove it.
No federal agency requires pharmacists to report medication errors, and few state boards of pharmacy mandate it. Many pharmacies and pharmacy chains track errors internally but do not share the numbers with the public. CVS and Walgreens both declined to share their data with USA TODAY.
“There really is no way of knowing how many errors are actually out there,” said Larry Selkow, a retired California pharmacist who recently served on the American Public Health Association’s task force on pharmacy medication safety issues.
The group estimated U.S. pharmacies annually make 54 million dispensing errors, of which 2.3 million are potentially harmful. It recommended the establishment of a national pharmacy reporting system to collect data on errors and their underlying causes. Having such information, Selkow said, would allow pharmacies to adopt practices to prevent future mistakes.
Numerous pharmacists told USA TODAY that errors are not consistently reported – even internally. Small mistakes and those caught early are routinely hidden.
“Some pharmacists don’t report it especially if they’ve already had, like, five errors that year," said Shane Jerominski, a California pharmacist who worked for both Walgreens and CVS. "For every error that gets found out, there will be an error that never gets caught."
Even when they do report potentially fatal errors, some pharmacists said, no one from their companies investigates how they occurred or makes changes to prevent them from repeating.
A former CVS pharmacy manager at a short-staffed, high-volume store in Georgia said he was horrified when one of his patients who was prescribed Bisoprolol for high blood pressure accidentally received a sleeping aid called Belsomra and got sick after she started taking it.
The pharmacist, who now works for Walmart, said he had hoped the error would be a wake-up call for higher-ups who might finally give his store adequate staffing. It didn’t work out that way.
“They had me do that little report, but my manager, nobody ever followed up,” he said. “They were like, ‘OK, cool, see if she would like a gift card, and we’ll handle it from here.’ And that was it. It’s like they could care less. Like it didn’t even happen.”
CVS did not comment on the incident, but Thibault said that the company’s first priority when it learns of any error is the patient’s safety. She said it then takes steps to correct the error and learn from it. Walgreens said in a statement that it’s mandatory for employees to report errors under the company’s “Continuous Quality Improvement Program.”
“We take any prescription error very seriously and have a multi-step prescription filling process with numerous safety checks to minimize the rare chance of human error,” said Marty Maloney, Walgreens’ senior manager of media relations.
Pharmacists are personally liable for medication errors and risk fines, discipline and loss of license if investigated and found responsible by their state board. Many told USA TODAY they get little or no support from their company when mistakes happen, even if the conditions imposed by those companies contributed to the error.
The Nevada Board of Pharmacy in September fined and suspended the licenses of two CVS pharmacists who accidentally gave a pregnant woman the abortion drug misoprostol instead of the fertility treatment she was prescribed. The mistake, which was first reported by 8NewsNow in Las Vegas, ended the woman’s pregnancy.
The Nevada board also fined CVS $10,000 over the objections of company attorney William Stilling who argued CVS itself did nothing wrong.
“The only allegation” against CVS, Stilling said, “is that they had these pharmacists.”
Pharmacy benefit managers played role in the current crisis
Retail pharmacy wasn’t always this bleak.
Twenty years ago the industry was thriving. CVS and Walgreens were opening new locations at a rapid clip. New pharmacy schools popped up to meet the needs of a profession in high demand. Meanwhile, Americans’ appetite for prescription drugs was soaring.
Independent and chain pharmacies alike were earning relatively healthy profits from drug sales and could afford to hire and retain enough staff to keep their operations humming.
A constellation of factors contributed to the industry’s downturn. They include rising drug costs, changing consumer habits and the emergence of online pharmacies.

But none looms larger than the outsized influence of pharmacy benefit managers. These third-party administrators of health insurers’ prescription drug programs have eroded the profits of retail pharmacies to the point where they now lose money on many sales.
“In today’s world, 7 out of 10 medicines dispensed by a pharmacy are dispensed at a loss,” Hogue said, referring to the non-generic drugs that represent pharmacies’ largest expense.
Pharmacy benefit managers, commonly referred to as PBMs, act as a middleman between the insurers, the drug manufacturers and the pharmacies. They negotiate drug prices with manufacturers, determine which drugs will be covered by insurance plans and set reimbursement rates for pharmacies that buy and sell the drugs.
As the power of PBMs rose over the years, they demanded bigger rebates from drug manufacturers and pocketed increasingly bigger shares of those savings instead of passing them along. They also lowered pharmacy reimbursement rates and tacked on hefty fees known as Direct and Indirect Remuneration.
The three largest PBMs – ExpressScripts, owned by Cigna; CVS Caremark, owned by CVS Health; and OptumRx, owned by the same company as UnitedHealthcare – control a majority of the market.
While PBMs’ collective profits skyrocketed over the past decade, their tactics plunged retail pharmacies into financial distress and left them scrambling for alternative sources of revenue, like vaccinations, to stay afloat.
The Federal Trade Commission launched an inquiry last year into PBM practices, which have already been the subject of several lawsuits.
Independent pharmacies have been hit especially hard. Not only are their reimbursement rates lower than those of chains, but their patients have been steered away by PBMs that insist they use a preferred chain pharmacy instead.
Charles Thompson, a pharmacist and independent owner of Grove Park Pharmacy in Orangeburg, South Carolina, said he has lost countless customers who were told by their PBMs to use CVS and Walgreens instead. Between that and the lower reimbursements, he said, Grove Park had to diversify to stay open. It now offers an in-store medical clinic, hospice services and medical equipment rentals.
“If I had to rely only on filling prescriptions,” Thompson said. “I would be out of business.”
Other independent pharmacies simply closed. The United States has lost more than 3,500 mom-and-pop pharmacies in the past decade, according to data from the National Community Pharmacists Association, which represents independent pharmacies.
“The independents have been the canaries in the coal mine,” said B. Douglas Hoey, chief executive officer of the National Community Pharmacists Association.
Now the chains are following suit. CVS, Walgreens and Rite Aid all recently announced the closure of hundreds of pharmacies as they face slumping revenues and the fallout from multiple lawsuits for their alleged roles in the nation’s opioid crisis. Rite Aid filed for bankruptcy earlier this month.
“It’s all coming home to roost,” Hoey said of the PBMs’ unchecked power and their practice of steering patients away from the independents and into the chains. “It has overloaded the system, and also that corporate mentally of just, ‘we’re going to work the workers to death,’ I think that’s coming home to roost, too.”
Pharmacists bleeding, crying, working alone
Like the metaphorical frog boiling in the pot, Wendy Lear said she didn’t realize how bad her job at CVS had gotten until there were so few staff left that she was forced to work alone, even when she had no business being behind the pharmacy counter.
Lear’s stint with CVS started in 2009 when the chain bought the independent pharmacy where she worked in Lexington, Kentucky. The transition was dramatic but initially tolerable, Lear said, because CVS retained enough pharmacists and technicians to meet the patients’ needs.
But that changed over the years as CVS whittled away its staff while heaping more work upon the few who remained.

One time, Lear recalled, she went to work while miscarrying her first child because her boss couldn’t find anyone to cover her overnight shift and begged her to go in. Bleeding, cramping and emotionally distraught, Lear said, she fielded phone calls and filled prescriptions until she had to lie down on the floor.
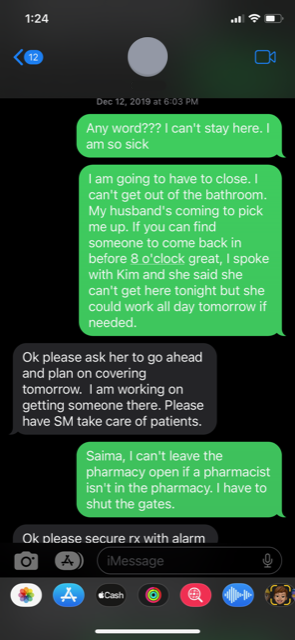
Another time when she was sick with norovirus and vomiting in a trash can behind the pharmacy counter, Lear said, she was asked to keep working until her boss could find someone to replace her. Lear toughed it out for two hours before texting her boss for an update.
“Any word???” she wrote. “I can’t stay here. I am so sick. I am going to have to close.”
Her boss texted back, instructing Lear to have the store manager take care of patients in her absence.
“That’s illegal,” Lear told USA TODAY of her boss’ request. “You have to have a pharmacist on premises to sell prescriptions. She was so frustrated I had to go home, and, it’s like, you have to have contingencies for when people fall ill during their shift.”
Eventually, Lear said, the demands of the job became too intense and the risk of errors too great – especially during solo shifts – that she quit CVS in 2021 and found a new job at an independent pharmacy, Remington Drug Co., in northern Virginia.
“Answering phone calls, taking prescriptions at drop off, entering those prescriptions, verifying once, filling those prescriptions, verifying twice, running the register, giving vaccinations, making metric-monitored phone calls, all fell on one person,” she said of her job at CVS. “In a double-check system, who’s checking me? This is when patient safety is most compromised.”
DeAngelis told USA TODAY it is not CVS’ policy or practice to require staff to work when they are ill.
But retail pharmacists from CVS and other chains across the country shared similar stories of corporate pressure and severe burnout:
- “All day long stuff’s blowing up and management is yelling at us because we can’t answer the phones fast enough and we’re not giving enough immunizations,” said a current Walgreens pharmacist in Arizona. “I’ve seen pharmacists cry back in the pharmacy because it’s so busy.”
- “This situation has slowly worsened, but the big turning point was when we started giving COVID shots,” said a current Walmart pharmacist in Iowa. “One day it was just me there, and I did 77 COVID shots.”
- “There was not a single week where I didn’t work 80 hours, but I was only paid 42,” said a former CVS pharmacist from Virginia. “We were behind on prescriptions the entire year. I was begging, ‘please can we get more hours?’ Instead, corporate would suggest we do these overnighters to get caught up.”
Thousands of retail pharmacists left the industry during the first two years of the pandemic, according to data from the Bureau of Labor Statistics, which reported a 6% drop in employment numbers between 2019 and 2021.
Although those numbers have rebounded to pre-pandemic levels, the latest data shows, overall interest in the profession has nosedived, raising questions about the future of pharmacy.
Applications to U.S. pharmacy schools plummeted nearly 70% from their peak in the fall of 2009 to the fall of 2021, according to the most recent data published by the American Association of Colleges of Pharmacy. Those schools, which graduated nearly 15,000 students a year at their peak, are expected to produce just 11,000 new pharmacists annually by 2025, Hogue said.
Stuart Beatty, dean of Ohio Northern University’s Raabe College of Pharmacy, said his school is facing the same enrollment slump despite efforts to recruit students and reassure them of a bright future.
If he and his academic peers can’t reverse the tide, he said, the nation soon could face a severe pharmacist shortage.
“It makes sense. Why would you go into a doctoral degree when all this is happening?” said Janan Sarwar, a Louisville-based pharmacist, publisher and career coach. “They want to help patients. They don’t want to enter a profession that oppresses their ability to help and do good in the world.”
Mistakes like this are why pharmacists say they're leaving
Shelby Richards blames chronic pharmacy understaffing for the medication error that cost her thousands of dollars.
The Memphis Walgreens she frequented was always “busy, low staffed, lines out the door,” Richards said, including the day in March 2021 when she retrieved a newly prescribed anti-anxiety medication to treat panic attacks after a car wreck.
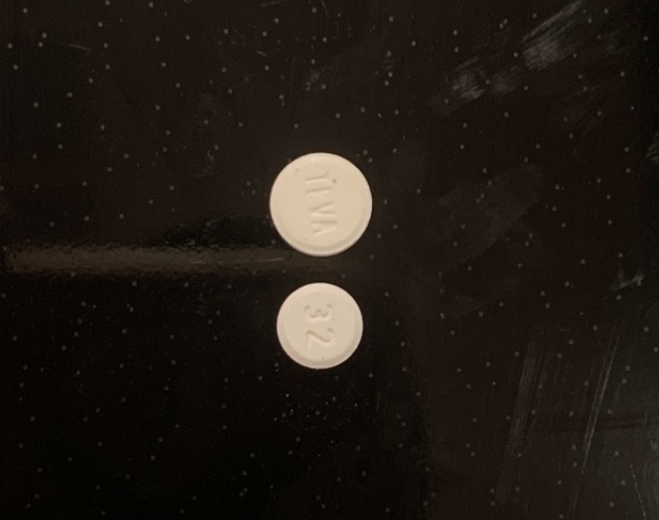
Inside the bottle were two sizes of round, white pills. Richards said she assumed they were different doses of the same drug because her doctor had mentioned wanting to start her on 5 mg of Buspar before increasing it to 10 mg.

So she started taking the smaller of the two pills, not realizing it was a different drug altogether – a calcium channel blocker called amlodipine to treat high blood pressure.
Within days, Richards said, she began to feel nauseous, light-headed and her legs were swelling – all common side effects of amlodipine. Uninsured, she racked up $15,000 in bills from three hospital visits as doctors tried in vain to determine the cause, records show.
It wasn’t until her boyfriend took a closer look at her medication and noticed the different-sized pills that she had an answer.
“I told her it … should always be a separate bottle,” said her now-husband Taylor Richards, who researched the two pills online and learned the one she had been taking was the highest dose of amlodipine available.
The couple called Walgreens to report the error and said they were dismissed without an apology. They tried to sue but missed the state statute of limitations, so they filed a complaint with the Tennessee Board of Pharmacy, which they provided to USA TODAY.
“It seems like their staff is working like slaves,” Taylor Richards said. “There are usually two people back there, and it’s probably one of the busiest pharmacies around. I imagine they’re requiring them to fill so many prescriptions that it will continue to cause these types of errors.”
Walgreens declined to comment on the error.

Pharmacists, meanwhile, said it’s a prime example of how working conditions put patients at risk and why so many of them are quitting the profession altogether.
It’s also why dozens of pharmacists recently walked out recently in protest. Another walkout is planned for Oct. 30-Nov. 1. Pharmacists are calling it Pharmageddon.
“The primary reason is our concern for public safety,” said Corey Schneider, one of the CVS pharmacists who participated in the Kansas City walkout. “It’s also about basic decency. Pharmacists shouldn’t have to cry at work or go home worried that they made a mistake.”
A few, like Tanoe, have funneled their frustration into advocacy. The former Walgreens pharmacist launched a public campaign in 2021 around the hashtag #PizzaIsNotWorking to highlight the dangerous working conditions that gestures such as free pizza from corporate won’t fix.
Since then she has connected with thousands of retail pharmacy workers through her Facebook page, LinkedIn account and the online pharmacist advocacy community, RPhAlly, of which she is the vice president. She also helped organizers of the recent CVS and Walgreens walkouts share their messages and recruit participants and supporters.
Tanoe said it’s time the state pharmacy boards, professional organizations and corporate owners take these concerns seriously. If not, she said, the nation will see fewer pharmacies, fewer pharmacists and more incidents of patient harm.
“For so long we have been told our patients come first – no matter what you do, your patient comes first,” Tanoe said. “Now, we are saying, no. We come first. We hold our patients’ lives in our hands. If we’re not well, they’re not well.”
Emily Le Coz is a reporter on the USA TODAY investigations team. Contact her at elecoz@usatoday.com or @emily_lecoz.
Disclaimer: The copyright of this article belongs to the original author. Reposting this article is solely for the purpose of information dissemination and does not constitute any investment advice. If there is any infringement, please contact us immediately. We will make corrections or deletions as necessary. Thank you.







